
Aortic Aneurysm
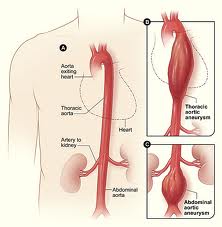
An aneurysm (AN-you-rism) is a protuberance or bulge in a blood vessel caused by weakness in the blood vessel wall. Aneurysms are dangerous because they may tear or rupture. The aorta is the body’s largest artery that carries blood from the heart to the rest of the body. On occasion it develops an aneurysm when the blood vessel wall is injured or weakened which may be caused by plaque or fat deposited on the blood vessel walls (atherosclerosis). Aortic aneurysms may occur throughout the aorta, from its origin, where it is joined to the heart, through the chest cavity (thoracic aortic aneurysm) and down to the abdomen (abdominal aortic aneurysm or AAA).
An aortic aneurysm is an enlargement of the aorta to roughly one-and-a-half times or more of its normal size. This can cause weakness in the aortic wall and the potential for rupture (much like an overinflated balloon), leading to massive internal bleeding and, unless immediately treated, sudden death. Although more common in men, women can also be at risk.
FAQ
Aneurysms may be caused by many underlying problems or associated with certain risk factors. These include:
- Atherosclerosis (also called arteriosclerosis)
- Hypertension (particularly persistently and poorly controlled high blood pressure)
- Injury in a blood vessel as a result of trauma (such as a car accident)
- Current or history of smoking (smoking for more than just a few years is a very strong risk factor, especially in men)
- Congenital abnormalities
- Aging
- Marfan’s syndrome (a genetic disease that causes abnormal weakness of the blood vessel walls)
- Overweight or obesity
- Family history of aortic aneurysm, heart disease or other disease of the arteries
- Use of stimulants such as cocaine
- Formation of atherosclerotic plaque at the site of the aneurysm
- Formation of a clot at the site, which subsequently detaches and can increase the likelihood of a stroke or damage to an organ or extremity.
- Increase in the size of the aneurysm, which causes pressure against other organs and causes pain
- Rupture or tearing of the aneurysm —because the artery wall becomes thinner in this place, it becomes fragile and can rupture when subjected to stress. Sudden rupture of the aortic aneurysm can be life-threatening. A tear of the aorta is known as an aortic dissection and is also a life-threatening emergency.
A small aneurysm (or mild enlargement) generally does not imply any short-term risk and may not cause symptoms. A doctor should examine it regularly to detect whether it is growing. Cardiologists, vascular surgeons or specialists and thoracic surgeons are often called upon to evaluate patients with any questions of an aortic aneurysm or enlargement. When aneurysms grow, pain in the area of the aneurysm is a typical symptom. The larger the aneurysm is, the more likely it is to rupture or dissect (similar to how a balloon ultimately pops when it gets too large).
A relatively common congenital abnormality is a bicuspid aortic valve where there are two aortic leaflets rather than the normal three. This can be associated with enlargement or dilatation of the aorta (especially the very first part of the aorta attached to the heart known as the aortic root).
An aortic aneurysm is a potentially fatal condition that claims the lives of approximately 150,000 people in the United States annually. Aortic aneurysms rarely produce symptoms and therefore individuals may be at risk without their knowledge. While the treatment has improved significantly in the last decade, it is much better to deal with it electively rather than emergently where the risk of death or significant morbidity is extremely high. Thus it is literally vital for those at risk to be screened to determine whether or not there is cause for concern.
Those at highest risk include men over age 65 who have ever smoked, anyone with a family history of aneurysms and men and women with certain hereditary or cardiovascular conditions, especially Marfan’s.
The standard screening test for those at risk is a screening ultrasound (abdominal aortic ultrasound for those at risk of an AAA and an echocardiogram for those at risk of a thoracic aortic aneurysm-both of these tests are performed in our office). If no aortic enlargement is seen, then it is unlikely there is a need for anything further to be done. If the aorta is enlarged, then depending on the size, it can be monitored over time for further growth or the patient can be referred to a specialist for possible repair.
The U.S. Preventive Services task Force released updated guidelines in 2014 calling for one-time ultrasound screening for men ages 65 to 75 who have ever smoked. For men with no smoking history, other risk factors should be considered, including high blood pressure, high cholesterol, obesity and a family history of or herditary condition predisposing to anuerysms. The guidelines also recommend considering screening of women ages 65 to 75 who have smoked or have these other risk factors.
Aneurysms are diagnosed through detection tests performed on patients with risk factors for developing them or upon being discovered by chance when a test is performed for unrelated symptoms. They may also be discovered as part of a physical exam when your doctor palpates a suspect area during the examination. An aneurysm can be detected through X-rays or with imaging techniques such as echocardiography, ultrasound, magnetic resonance (MRI) or computerized tomography (CAT scan). If the aorta is mainly enlarged at the first part, or root, right above the heart, often an echocardiogram suffices to follow it up over time. If other parts of the aorta are enlarged, often a CT scan or MRI is necessary to visualize the aorta adequately. Because a prior or current history of smoking (more than just for a few years in the past) is such a strong risk factor for developing an abdominal aortic aneurysm (AAA), often a special type of abdominal ultrasound, known as an abdominal aortic duplex can be performed to make sure that there is no unusual enlargement or aneurysm of the abdominal aorta. This is a painless and non-invasive test with no radiation involved that usually takes less than 15 minutes and is performed in our office.
Once an aneurysm is discovered, the treatment depends on its size and location. It is possible to administer medications to lower blood pressure and try to delay the growth of small aneurysms. Aneurysms are surgically treated when they grow to the point that the risk of rupture or dissection is greater than the risk of performing surgery. The aneurysm is removed and replaced with a graft, which is an artificial substitute for the damaged portion of the aorta. If the aneurysm is close to the aortic valve (the heart valve that separates the aorta from the heart), replacement or repair of the valve often needs to be considered.
In patients with a bicuspid aortic valve who also have aortic root enlargement need regular imaging (usually with echocardiography) over time (if the ascending aorta diameter is over 4.0 cm) with surgical repair if the ascending aortic diameter is greater than 5.0 cm or is increasing more than 0.5 cm/year. It is also often recommended to repair the ascending aorta at the time of aortic valve replacement if the diameter of the aorta is greater than 4.5 cm.
Evolving newer techniques to repair aortic aneurysms with less invasive endovascular procedures and stenting (EVAR – endovascular aortic repair) rather than actual surgery are being developed and are used in appropriate patients at centers with adequate experience. In the last decade there has been growing use of technology to make the reparative treatment less invasive with patients now often going home often within a day or two rather than over a week after traditional surgery. For abdominal aortic aneurysms, the majority of patients now have anatomy suitable for a less invasive stent graft endovascular repair rather than open surgery.
Click here for more information on aortic aneurysms.
Updated 09/18/15
Written by and/or reviewed by Mark K. Urman, M.D. and Jeffrey F. Caren, M.D.
PLEASE NOTE: The information above is provided for general informational and educational purposes only and should not be used during any medical emergency. The information provided herein is not intended to be a substitute for medical advice, nor should it be used for the diagnoses or treatment of any medical condition. Accordingly, it should not be relied upon as a substitute for consultation with licensed and qualified health professionals who are familiar with your individual medical needs. Call 911 for all medical emergencies. Links to other sites are provided for information only they do not constitute endorsements of those other sites. Please see Terms of Use for more information.